CapsoVision for Capsule Endoscopy
The CapsoCam Plus System is a sophisticated, user-friendly capsule endoscopy solution that provides a full 360° image of the small bowel mucosa – the most comprehensive capsule endoscopy visualization available on the market.
The thorough imaging of the CapsoCam Plus System is enhanced by its wire-free design, which allows for flexibility in patient scheduling, while also providing unprecedented patient freedom and comfort during the examination.
CapsoCam Plus
Now with higher resolution and double the memory, CapsoCam Plus provides the most comprehensive imaging available in capsule endoscopy.
Developed with Silicon Valley innovation, the all-new CapsoCam Plus System is a state-of-the-art, user-friendly capsule endoscopy solution that is designed, tested, and packaged in the U.S.A.
CapsoCam Plus is designed to improve diagnostic confidence by providing a full 360º panoramic lateral view of the small bowel mucosa. More detailed imaging and a larger vertical field of view allow for better tissue characterization than previous generations of CapsoCam.
Higher Resolution. Greater Clarity.
The imaging hardware in CapsoCam Plus has been redesigned and optimized to deliver a more thorough view of the small bowel mucosa. With higher resolution and double the memory, CapsoCam Plus provides the most comprehensive imaging available today. More detailed imaging allows for greater diagnostic confidence.

Ampulla of Vater

Crohn’s Disease

Ectasia

Melanoma

Submucosal Mass
What You See Is What You Get
End-facing cameras have an inherent limitation in imaging the inner curvature of the intestinal wall. In fact, the inability of these older capsule endoscopes to visualize interior landmarks such as the ampulla of Vater is well documented.1 Studies have shown that faster frame rates and a wider field of view do not overcome this limitation, which could account for missed lesions elsewhere in the small bowel.2
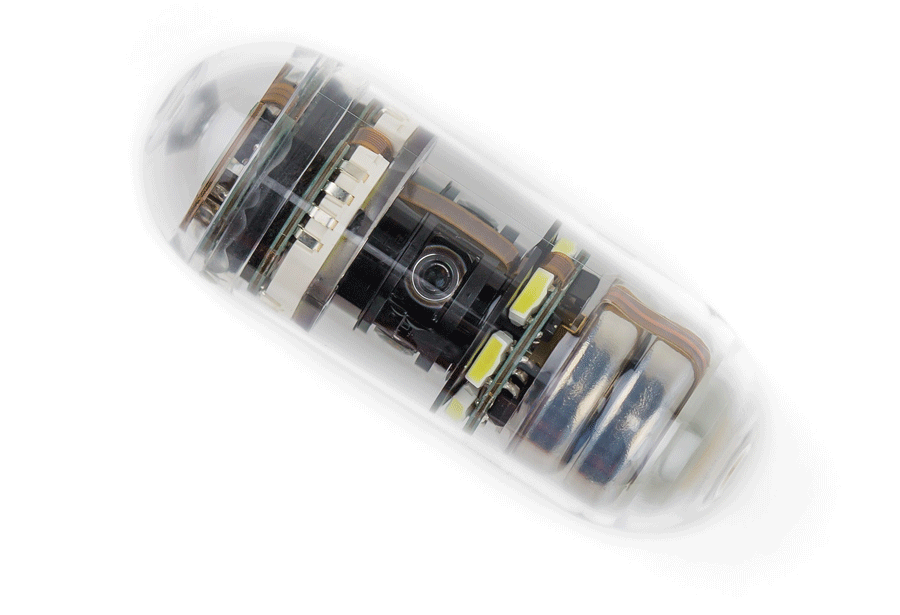
The value of end-facing cameras is further limited by tumbling, incomplete illumination and the inability to visualize behind mucosal folds. CapsoCam Plus overcomes these barriers by using four lateral, on-board cameras that capture high resolution 360º images of the small bowel, providing a detailed examination of the mucosal surface.
CapsoCloud®
Introducing CapsoCloud™, the only exam management system that allows you to extract data from the CapsoCam Plus capsule without the need to process capsules post-ingestion. HIPAA-compliant and secure, CapsoCloud gives you easy access to your patient’s exam data at your convenience.


A user-friendly portal that takes you right to the review.
You already see more with the CapsoCam Plus 360° lateral view of the small bowel mucosa. With the CapsoCloud portal, downloading patient videos is simple, yet secure.
Swallow to Screen in Four Simple Steps:
Step 1: Patient swallows the CapsoCam Plus capsule in your office.
Step 2: Patient excretes then retrieves the capsule at home and ships it in a prepaid return label envelope to the CapsoCloud Download Center.
Step 3: The CapsoCloud Download Center processes and uploads the video to the secure, HIPAA-compliant portal.
Step 4: You access the video via the CapsoCloud portal and download the patient results.
CapsoCloud in the News! –
Formal Press Release – A formal press release went out announcing the launch of CapsoCloud to all US medical device and financial wires. We’ve included this release as well as new content on our website and all social media channels. This is a game-changing product that will save time and resources for gastroenterologists using capsule endoscopy.
News Outlets who have picked up our press release:
Online Magazine Article – Great news! We have our first magazine article on CapsoCloud! The print version of Healio Gastroenterology has a paid, online and print circulation of over 15,000. This is in addition to casual web traffic! It’s likely this will run online only, but even so, it will get plenty of views!
More News Magazine Articles:
Clinical Evidence
While CapsoCam Plus® has been proven to be a safe and effective diagnostic tool, ongoing research and clinical evaluations continue to expand the range of clinical indications.
Below you will find the clinical outcomes from international studies performed with the CapsoCam small bowel capsule endoscope.
The duodenal papilla as quality criterion of small bowel capsule endoscopy.
CapsoCam– A newly developed small bowel capsule endoscope with 360° view.
Andreas Sieg, M.D. Ph.D. (1)(3) and Sven Genhrke, M.D. Ph.D. (1)(2) (1) University of Heidelberg, Dept. of Gastroenterology, (2) Practice of Gastroenterology- Baden, (3) Practice of Gastroenterology- Heidelberg
Introduction
Capsule endoscopy has evolved to become a first-line, noninvasive diagnostic technique for the small bowel. However, the inability to visualize the duodenal papilla is an inherent limitation of this method. We evaluated the diagnostic yield and completeness of the small bowel examination with a newly developed video capsule (SV1, Capsovision, Saratoga, CA) with panoramic 360° imaging.
Methods
SV1 is a small bowel video endoscope measuring 11×31mm capturing colour high-resolution images at 4 frames per second in a 360-degree-panorama-view for the first 2 hours and 3fps for the rest of time. This enables a side view like with ERCP. The device does not employ wireless technology. SV1 saves the data on the on-board flash memory when it traverses through the bowel. The capsule is retrieved, opened by the docking station where the data are transferred by USB to the reviewing workstation. 24 patients (13 F and 11M, mean age 45 y) in whom evaluation of the small bowel was indicated swallowed SV1 either after colonoscopy or after a preparation with 2l of a PEG solution in the afternoon before the examination. The patients swallowed 20mg of metoclopramide and 170mg of simethicone 30min before swallowing the capsule. They were allowed to eat after 6 hours.
Results
The capsules were retrieved in 23 of 24 patients forming the study population. One patient lost its capsule. The mean time to pass the stomach was 24min and the small bowel 234min. The duodenal papilla was identified in 15 of 23 patients (65%). We further detected mucosal breaks/ulcers in 5 patients with Crohn’s disease, in 1 patient with NSAR use and in 1 patient with anemia. No adverse effects were detected.
Discussion
Compared to capsules with cameras at the end, SV1 with a 360° imaging detects the duodenal papilla in a higher proportion which is an advantage for the diagnosis of neoplasms of the papilla and duodenum. We also detected pathologic findings in the lower part of the small bowel. Every capsule reached the ileocecal valve. Small bowel capsule endoscopy with SV1 is a safe procedure. The panoramic imaging capsule seems to have an advantage in small bowel.
Prospective randomized multicenter comparison of two intestine capsule endoscopy systems with lateral view and axial view in obscure digestive bleeding situations.
J.C. Saurin, M. Pioche, G. Vanbiervliet, P. Jacob, C. Duburque, R. Gincul, B. Filoche, J. Daudet, J. Fillppi, T. Ponchon, M. Pioche, G. Vanbeirvllet, P. Jacob, C. Duburque, R. Ginc Sociéte Française d’Endoscopie Digestive (SFED). (1) Lyon; (2) Nice; (3) Nîmes; (4) Lille. February 2013.
Overview
The 360 degree panoramic view of the CapsoCam provided superior lesion detection. This could be of practical value in patients with a large number of lesions. The CapsoCam identified a significantly higher number of lesions compared to the Pillcam SB2 – 107 Capsovision identified lesions versus 85 Pilcam SB2 identified lesions, a 29% increase in diagnostic yield.
Introduction
A multicenter, randomized, prospective evaluation of the small intestine capsule with 360 ° lateral view CapsoCam from the company CapsoVision ° (4 side cameras) versus capsule endoscopy system Pillcam SB2 from the company Given Imaging was performed.
Patients and Methods
Four French SFED centers were included (Lille, Lyon, Nice, Nîmes), patients presenting obscure gastrointestinal bleeding (externalized bleeding or anemia). Each patient ingested in randomized order, 2 capsules at 1 hour intervals. The capsule CapsoVision must be retrieved during excretion and returned to the operator for film analysis. The capsule films were read by one of the two reading systems present in each center. The study’s main objective was based on the concordance of results (k>0.60). Secondary objectives were the sensitivity per patient and the sensitivity per lesion.
Results
73 consecutive patients were included. Thirteen technical failures occurred: 5 capsules not returned by patients, 5 films nonanalyzable, 1 capsule non ingested (Capsovision °) 1 capsule non ingested and 1 film non analyzable (Given). Of the 60 remaining patients analyzable, there were 22 (36.6%) cases of positive concordant diagnosis, 27 (45%) negative concordant diagnosis, and 11 (18.3%) were discordant (6 times in favor of Given Imaging °, 5 times in favor of CapsoVision, 4 ulcerations, 5 angiodysplasia, 1 polyp, 1 active bleeding). The concordance between the 2 examinations was good (main objective): k = 0.63 analyzable, k = 0.60 by intention to treat (itt). The rate of diagnosis sensitivity per patient (in itt and per-protocol) was comparable for the 2 capsules (29/73 positive diagnosis CapsoVision versus 31/73, p = 0.79), with an analysis by lesion, a higher number of diagnostics (mainly angiodysplasia) were identified by the CapsoVision capsule (108 CapsoVision versus 85 Pilcam SB2 , p <0.01). The average reading times were 32.0 minutes (Capsovision °) versus 26.2 min (Given °).
Conclusion
With a kappa value of 0.63, this study shows that the capsule CapsoCam enables exploration of the small intestine with the same diagnostic performance as the capsule PillCam SB2 currently used by most French centers. Superiority of the capsule providing a lateral image of 360 ° even appeared on the number of lesions detected. This could be of practical value in patients with a large number of lesions for which the number is significant (monitoring of Osler Weber–Rendu disease for example). On the other hand, the need to recover the capsule to return it in order for the recorded films to be transferred to the reading systems is a limit responsible for 5 of the thirteen failures that occurred in the study with this material. It is therefore an effective system, with a time of close reading that can fit into the arsenal of techniques for exploration of the small intestine.
Experience of Video Capsule CapsoCam in 2 centers.
H. Blasco-Perrin (1), G. Galindo (1)(2), A. Reffet (3), J.L. Payen (1) (1)Pôle médico-chirurgical du CH de Montauban (2) Clinique du Dr. Boyé Montauban (3) Service de maladie digestive et tropicale, Hôpital Robert Picque, Villenave-d’ornon.
Overview
CapsoCam is easy to use (no external sensor). Its efficacy seems comparable to PillCam SB2. The CapsoCam capsule can be effectively used on the diagnosis of patients with occult bleeding or suspected Crohn’s disease in the case of negative endoscopic exploration. The 360 degrees lateral panoramic view provides improvement in the detection of angiodysplasia.
Methods and Materials
We included 38 patients between January and October 2012, under the following criteria: – All the patients were referred to our 2 centers – for iron deficiency anemia (Group 1) or suspected Crohn’s disease (Group 2) – negative endoscopy results (gastroscopy and colonoscopy with normal ileoscopy) The patients were diagnosed by the video capsule CapsoCam with the following characteristics: 4 cameras, 360 ° panoramic view, data stored in the capsule. The indication was consistent with the criteria for reimbursement of the act by the CPAM. A 1st consultation enables the explication of the preparation modalities : liquid meal the day before, one sachet of Citrafleet ® at 18H00 the day before and at 7H00 the morning of the day of ingestion of the capsule, fasting of the patient, as well as the recovery method of the capsule.
Results
38 patients were consecutively included in the study, 21 in group 1 and 17 in group 2, average age 66.5 years respectively + / – 34.5 years and 39.9 + / – 28. The detection rates were respectively 47.6% and 58.8% (see Table 1). There were 3 procedure failures (8.3%): – 2 early apparitions of alimentary bolus – 1 due to the lack of recovery of the capsule There was no capsule retention 50% of gastrointestinal bleeding of unknown origin was due to small bowel angiodysplasia, 18% due to celiac diseases of small intestine tumors.
Conclusion
This video capsule is easy to use (no external sensor). Its efficiency seems comparable to the main competitor. The CapsoCam capsule appears to have its place for the exploration of patients with occult bleeding or suspected Crohn’s disease in the case of negative endoscopic exploration.
Extensive small-bowel Crohn’s disease detected by the newly introduced 360° panoramic viewing capsule endoscopy system
Gian Eugenio Tontini, Flaminia Cavallaro, Helmut Neumann, Luca Pastorelli, Markus F. Neurath, Luisa Spina, Maurizio Vecchi, Gastroenterology and Digestive Endoscopy Unit, IRCCS Policlinico San Donato, San Donato Milanese, Italy Department of Medicine I, University of Erlangen-Nuremberg, Erlangen, Germany Department of Biomedical Sciences for Health, University of Milan, Milan, Italy
Chronic, nonbloody diarrhea may represent a diagnostic challenge in patients with inconclusive findings after standard clinical work-up [1]. In this setting, smallbowel capsule endoscopy (SBCE) has high sensitivity and a favorable clinical impact in assessing the presence of small-bowel mucosal lesions in patients with suspected Crohn’s disease and no obstructive symptoms [1–3].
Very recently, the CapsoCam SV-1 (CapsoVision, Inc. Saratoga, California, USA) has been introduced as a new standard in SBCE. The system allows lateral panoramic 360° viewing with wire-free technology, long lasting battery life, and 12–20 frames per second captured by four highresolution cameras located on the capsule sides and facing the four quadrants of the digestive wall [4, 5]. To the best of our knowledge, there is no published report on the use of this new technique in patients with suspected small-bowel Crohn’s disease. Here, the case of a 51-year-old woman with a 2-year history of chronic, nonbloody diarrhea is presented. Physical examination was unremarkable and laboratory parameters were within the reference ranges, with the exception of a low albumin level (3 g/dL). Non steroidal anti-inflammatory drug use, infectious disorders, and gluten and lactose intolerance were ruled out. Previous upper and lower endoscopy with biopsies and abdominal cross-sectional imaging did not reveal any lesions. A second ileocolonoscopy showed subtle ileal erosions with histopathological evaluation that was inconclusive for Crohn’s disease. It was decided that SBCE with CapsoCam SV-1 should be performed. The patient swallowed the capsule as directed and retrieved it 52 hours later.
The wire-free capsule system was then inserted into the bench storage device and the on-board data were downloaded using a standard computer. The SBCE video record provided high quality, four quadrant images (n=3650) for the whole duration of the recording (total recording duration 14 hours; transit time, gastric 57 minutes, small bowel 202 minutes). An impressive number of erosions (n=27)
and ulcers (n=97) from the distal duodenum to the terminal ileum were observed (Figs.1–4; Video 1). All lesions occurred among normal-appearing mucosa, with no trace of strictures. The 360° panoramic view, together with the high rate of recorded frames, allowed for a clear characterization of each lesion. A remarkable number of frames were recorded per erosion or ulcer (mean 7 frames [range 2– 14] per erosion, 9 frames [range 3–33] per ulcer), and distinct perspectives of lesions were captured by each camera (mean number of cameras capturing the lesion, 1.5 [range 1–3]). This feature represents a tangible improvement in lesion classification and differential diagnosis (i.e. for classification of the lesion type or distinction between different or redundant findings). Based on these findings, the diagnosis of extensive small-bowel Crohn’s disease was made and the patient improved with specific therapy.
This case is interesting for several reasons. First, an unusual case of extensive luminal small-bowel Crohn’s disease was identified
in a patient with a long history of chronic, nonbloody diarrhea. Second, the report adds to the growing literature on advanced endoscopic imaging techniques for the small bowel [1–3]. Finally, the performance of a new standard for SBCE has been described, providing multiple, high resolution images and visualizing different aspects of each lesion, which have the potential to improve both the diagnostic yield and the confidence of the operator in assessing the diagnosis and the differential diagnosis.
These studies were conducted outside the U.S. and any results have not been evaluated by the U.S. Food and Drug Administration (FDA).